

Introduction
Polycythemia vera (PV) is a myeloproliferative neoplasm characterized by the increased red cell mass and high thrombotic risk. The main objective of therapy is to maintain the hematocrit <45% with hydroxyurea (HU) being the most common drug employed in first line. Patients developing resistance/intolerance to HU are at higher risk of thrombosis due to inadequate hematocrit control.
Methods
This ongoing phase 4 observational study recruited 352 patients with PV resistant and/or intolerant to HU treated with ruxolitinib (RUX), with a follow-up of 24 months after treatment initiation. In the present interim analysis, 150 patients with PV receiving RUX treatment for 52 weeks were evaluated for efficacy and safety parameters. Inclusion criteria were adult patients aged ≥18 years diagnosed with PV resistant/intolerant to HU (as per European LeukemiaNet [ELN] criteria) treated with RUX according to the approved local label. RUX treatment could be initiated up to 6 months before inclusion. The informed consent was obtained from all patients. The myeloproliferative neoplasm symptom assessment form total symptom score (MPN-SAF TSS) and the pruritus symptom impact scale (PSIS) were employed for symptom evaluation.
Results
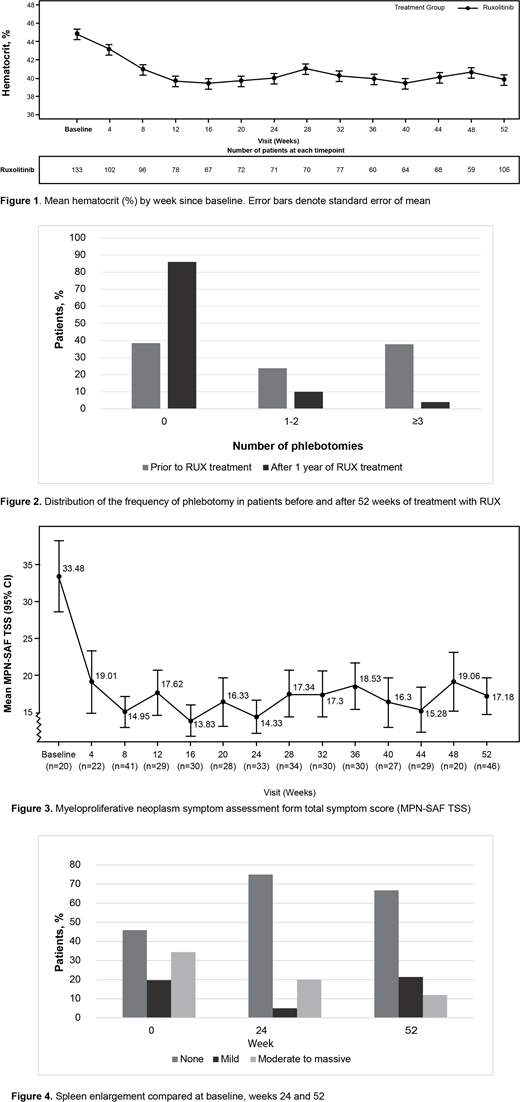
Of the 150 patients included, 67.3% were aged >60 years and 51% were males; 61% were resistant to HU and 65% were intolerant to HU. The median duration of PV was 67 months prior to the study entry. The medical history of patients included thromboembolic events (TEs) in 29.3%, infections in 18.6%, secondary neoplasms in 12.6%, and bleeding in 5.3% of patients. At baseline, TEs were present in 17.3% of patients, infections in 10.6%, secondary neoplasms in 6%, and bleeding in 2% of patients. Hematocrit was measured in 133 patients at baseline with inadequate hematocrit control being observed in 62 patients (47%): >45% to <48%, n=28; ≥48%, n=34. The proportion of patients dependent on 1 to 2 and ≥3 phlebotomies 1 year before the RUX treatment were 24% and 38%, respectively. Hematocrit levels dropped from week 8 to 12 to a sustained mean value of 40% during the observational period (Figure 1). The dependency of patients requiring 1 to 2 and ≥3 phlebotomies decreased from 24% and 38% at baseline to 10% and 4%, respectively after 1 year of RUX treatment (Figure 2). The mean MPN-SAF TSS declined rapidly from a score of 33 at baseline (n=20) to 19 (n=22) upon the treatment initiation and evolved to stabilize at week 16 (n=30) throughout the observation period (Figure 3). On mean PSIS, a rapid decline in severity of pruritus (past 7 days) from 5.20 at baseline (n=15) to 0.95 (n=20) after 4 weeks of treatment was observed. The effect of RUX treatment on patients with moderate and massive splenomegaly was observed as early as 4 weeks after the treatment initiation. The proportion of patients with moderate-to-massive splenomegaly was reduced from 34.4% at baseline to 11.9% at week 52, while the proportion with no splenomegaly increased from 45.9% to 66.7% (Figure 4). Patients received a mean daily dose of 21.1 mg RUX. The majority of patients (89%) did not have dosing interruptions, and 11% had only 1 dosing interruption. The dose increases were more prominent than the decreases (53% vs 37%, respectively), and the majority had only 1 dosing increase or decrease. Adverse events (AEs) reported during the study included infections in 43.3%, TEs in 10%, secondary neoplasms in 6%, and bleeding in 10% of patients. Grade 3 to 4 AEs reported during the study included infections in 4.6%, TEs in 2%, secondary neoplasms in 1.3%, and bleeding in 0.6% of patients.
Conclusion
In this phase 4 observational study, RUX treatment achieved hematocrit control in a majority of patients with PV who were resistant/intolerant to HU and was associated with a low rate of grade 3 to 4 TEs. Additional benefits included symptom improvement and reduction in splenomegaly. The safety, particularly regarding infections and secondary neoplasms, will be further explored during the final analysis of the study.
Gisslinger:AOP Orphan Pharmaceuticals AG: Honoraria, Research Funding; Novartis: Honoraria, Research Funding; PharmaEssentia: Honoraria; MyeloPro Diagnostics and Research: Honoraria; Janssen-Cilag: Honoraria; Roche: Honoraria; Celgene: Honoraria. Devos:Novartis: Consultancy, Membership on an entity's Board of Directors or advisory committees. Lippert:Novartis: Other: Personal fee, Research Funding. De Stefano:Novartis: Other: Personal fee, Research Funding; Amgen: Other: Personal fee; Bayer: Other: Non-financial support; Celgene: Other: Non-financial support, personal fee; Janssen Cilag: Other: Non-financial support. Dahm:Novartis: Other: Reimbursement of study costs and personal fee; Pfizer: Other: Personal fee, Research Funding; Bristol-Mayer Squibb: Other: Personal fee; Bayer: Other: Personal fee; MSD: Other: Personal fee. Zuurman:Novartis Pharma A.G.: Current Employment. Zaiac:Novartis: Current Employment, Current equity holder in private company. Houtsma:Novartis: Current Employment. Iqbal:Novartis: Current Employment. Di Matteo:Novartis: Current Employment.

This feature is available to Subscribers Only
Sign In or Create an Account Close Modal